

Why is everyone suddenly on steroids? (And should you be?)
The secret shopper study found 85% of online clinics prescribe testosterone to people who it may permanently harm.

GQ magazine recently ran a trend story: WHY IS EVERYONE SUDDENLY ON STEROIDS?
My good friend and one of my favorite writers—Foster Kamer of FOSTERTALK—saw that coverline and had a great insight, writing:
Like all trend stories, it deserves to be turned upside down and investigated for sport like it’s Watergate, so: I called a friend who’s been taking steroids on and off starting in his mid-30s. Super successful, lovely guy — perhaps, among the nicest I know — and also, built like a brick shithouse.
What followed was one of the funniest yet rawest and most and informative Q&As I’ve read in years.
Foster published the conversation on his great Substack, FOSTERTALK (which you should check out). He’s graciously allowed me to re-run the conversation on Two Percent.
Here’s today’s roadmap:
Foster talks to a steroid user: A raw, unfiltered, Q&A with a successful professional who started taking steroid-like drugs (TRT, SARMs, etc) in his mid-30s (and what happened to his body).
The facts on TRT: I’ll break down the surging world of TRT and what you should know about it.
The online clinic problem: What Northwestern University’s “secret shopper” study exposes about how 85% of online clinics operate.
Who TRT is good for: A clear framework on who it actually helps — and the specific risks for everyone else.
Housekeeping
This post, like all Monday posts, is free to all subscribers. Only Members get full access to all three weekly Two Percent posts, audio versions, and our entire archive. Become a Member:
Weekly Recap:
On Wednesday, we gave you the only rucking calorie calculator you’ll ever need, backed by military science. Plug in your numbers, get your results.
Friday’s Gear Not Stuff featured 13 essential travel items that I’ve tested across hundreds of thousands of miles.
Thanks to our partners:
GOREWEAR. I used GOREWEAR gear on a long and rainy hike over the weekend. Specifically, the award-winning CONCURVE GORE-TEX Jacket which kept me dry and fast. Check it out. EASTER gets you 30% off your first GOREWEAR purchase. It’s pure Gear Not Stuff.
Maui Nui harvests the healthiest protein on planet earth: wild (and invasive) axis deer on Maui. The nutritional value of axis deer is incredible. Check out the Mahalo Sale, which is offering 35% off of select cuts. Head to mauinuivenison.com/lp/EASTER to secure access.
Audio Version
Here’s Foster’s conversation:
Is Everyone (Actually) on Steroids, And Also, Should I (and You) Be Taking Them? A Q&A With an Anonymous Friend Who Took Steroids …
Foster: Is everyone suddenly on steroids?
Anonymous: Suddenly, no. Everyone? Well, in the sense that you know way, way more people than you think are doing them, yeah [laughs], for sure.
F: Wait, really?
A: It’s especially true of the New York/LA professional set, where you’re dealing with an ambitious crowd with a little bit of extra income, and boom: High likelihood if you think they’re doing it — if they’re not just losing weight (Ozempic) but getting in great shape — they’re doing it. Or doing something like it. Maybe it’s not TRT, maybe it’s Clomid. But it’s something.
F: Is this one of these things where — like SSRIs or ADD drugs or Zempies — there’s a stigma attached, but the moment you start talking, everyone…
A: … Admits to being on them, too, yeah, exactly. You have a few conversations, start going down the rabbit hole, and it’s: Holy shit, how many people are doing this?
F: What originally prompted you to go on them?
A: Honestly: Depression. I tried therapy and antidepressants. I’d always had low energy. And I’d heard good things.
F: I mean, my guy, you’re very, very in shape sans-roids. And a good-looking sweetheart of a man. With a great career. I should note, for our readers, that you’re the only person I know to have not one, but multiple strippers try to wife you. As in, give you their number because they want to date you. You’re the opposite of the T-Pain song, you’re the Yakov Smirnoff joke of strip clubs: YOU don’t love strippers, strippers love YOU.
A: Okay, well, that was be—
F: You’re like the guy who goes into a casino every once in a blue moon and wins a million dollars — you inspire all the other gamblers.
A: That’s not really wh—
F: Lemme ask you: What’s it like to have a woman see you, your career, your good family, your values, your picture-perfect health, and think not I can fix him but rather I wonder how I can break him?
A: What.
F: Steroids! What’d you take and how illegal are they?
A: The thing is: You don’t get anything illegally if you work with the right doctor. You can get anything prescribed. Off-label use is just one routine workaround. As for what I took, it was 80/20 testosterone and human growth hormone. And then you start stacking things on top of it to balance all the drugs out.
F: Sounds onerous. But on a scale of pretty fun to extremely fun, how much fun are steroids?
A: The first six months were amazing. I felt energized. I radiated positivity all the time. I was happy — I felt the way I thought I should feel, I felt emotional textures more distinctly, I felt things so much more strongly. And my sex drive was through the roof. Then what happened was… you get side effects.
F: Famously so! What’re we talking?
A: Depression. I became very, very emotional.
F: Roid rage?
A: It wasn’t so much rage as it was…
F: You wanted to jump off a building?
A: I mean, yes.
F: Hm. Not great. Gotta ask: Your balls, they get small?
A: …Yes.
F: How small?
A: Small.
F: Sure, but—
A: Really small.
F: On a scale of M&Ms to Jawbreakers?
A: I mean, they probably…[considers this deeply]
They were probably a third of the size. It got, like, uncomfortable. It felt weird.
F: I’ll say. And that’s not even why you were going crazy! Those were just small balls!
A: Right.
F: So, the big takeaway, here, is that all these guys writing for men’s magazines and going on podcasts and talking about their kettlebell routines have teeny tiny testes?
A: If they’re on steroids, probably.
F: Now there’s an image. What else you got?
A: For the record, the “man boobs” phenomenon is also real, but I didn’t experience that—though I was carrying some extra water weight. You take these drugs to inhibit/counteract your estrogen and suppress it. One of them was legitimately a cancer treatment drug.
F: What.
A: Yeah. It was a minor form — a pill, chemo in pill form. And it just wrecked my body. It got to the point where my joints were sore all the time. I felt horrific.
F: Well, that’s f*cked. You eventually got off them and deflated like a balloon.
A: Thanks.
F: What happened?
A: The 2020 COVID lockdown. I couldn’t lift weights because I was stuck in the apartment, and all I could do was run. So I went from eating 4000 calories a day and lifting heavy weights five days a week to: At home. Eating. So I cut my calories in half.
F: And do you still take anything now?
A: I’m taking this stuff called HCG, which is sort of like a testosterone precursor. And I think it just helps, because it’s not straight-up TRT, it doesn’t throw everything else out of whack. In hindsight, I kind of wish I had just started off being on that, rather than starting in the deep end, but it was a learning experience, and it’s really cool to sort of see what you can turn your body into.
F: Now, to the important part: Steroids, would I enjoy them?
A: [Laughs] You would definitely enjoy them.
F: So should I do them?
A: If you want to do them, I’d probably start with something small. First, Clomid or HCG, or Testrol, something a little bit more mild would be probably my suggestion.
F: So…not pure testosterone.
A: Not unless you really need it.
F: I still enjoy the occasional Broadway musical, so.
A: The honest truth is that it’s fun, but I wish my doctor started me on something less. That’s what I’d tell people: Start slow.
F: Like, not with Sondheim.
A: What?
F: Steroids! The Musical?
A: What.
OK, now back to Michael, pulling you out of the weird and wonderful mind of Foster and into some science …
As our anonymous source noted, there’s a constellation of “steroid-ish” drugs1 that men are using for a range of goals: more muscle, more energy, less fat, more sex drive, and more “vitality,” whatever that means.
There are growth hormone-related compounds, selective androgen receptor modulators (SARMs), and more. Because testosterone replacement therapy (TRT) is most common, we’ll focus on that:
What is testosterone?
I’ll quote some Johns Hopkins2 researchers: “Testosterone is a hormone produced in the Leydig cells of the testicle and is responsible for male sexual differentiation and development. While locally produced, testosterone affects the entire body, regulating sex drive, bone mass, fat distribution, muscle strength as well as various other bodily functions.”
It’s also linked to behavior—e.g., risk-taking, mate-seeking—and its impacts are more prevalent in males.
How does TRT work?
Humans have been messing with testosterone for a long time. The Roman scientist and thinker Pliny the Elder recommended that men eat animal testicles to alleviate symptoms of fatigue and erectile dysfunction.
It wasn’t until the 1920s that scientists isolated the hormone testosterone. And, from there, experimentation exploded.
Modern testosterone replacement therapy is simply giving the body a manufactured form of the hormone to supplement or replace the body’s natural testosterone.
You typically take the testosterone via injections, creams, patches, gels, or pills.
Why are people taking it?
Once we’d isolated testosterone in the 1920s, doctors used it for all kinds of insane reasons: to “treat” homosexuals, believing hormone imbalances caused homosexuality; to deal with psychiatric disorders, which led to irreversible changes in women. By the 1950s, it was being used by the East Germans as a performance enhancing drug.
Eventually, doctors realized that TRT was very useful for a narrow group: men who had clinically low testosterone levels (often from medical issues like androgen deficiency, hypogonadism, etc)3.
Those Hopkins researchers noted, “when used appropriately (TRT) can significantly improve the quality of life for men with testosterone deficiency.” Bringing low testosterone levels up into a more “normal” range coincides with improvements in bone density, mood, sex drive, muscle mass, and more.
Then came the wellness wave.
TRT started being marketed to men who had all sorts of vague problems that are part of everyday life. Low energy? Low libido? Grumpy? Aging? Not as jacked as you’d like? TRT, TRT, TRT, TRT, TRT (or HGH, SRAMs, etc).
Friend of Two Percent, Adam Cifu, MD, calls this “cosmetic medicine,” and explained in a Sensible Medicine article: “This is the type of medicine practiced when a doctor gives a name to a symptom that is part of the human condition (fatigue, achy muscles, grief, loss of libido, dysthymia…) and medicalizes it, offering a treatment, usually without evidence that the treatment even helps.”
Sales surged.
Are those problems all caused by low testosterone?
For most people, no. Some men have low testosterone but don’t have symptoms. Having both clinically low testosterone and symptoms is rather rare. It impacts anywhere from 2 to 8 percent of men age 40 to 80, depending on which study4 you read.
Most symptoms men and clinics blame on low testosterone stem from behaviors, not a hormone deficiency. For example, not enough sleep, too much work and family stress, drinking too much, obesity, medications like SSRIs, overtraining, etc.
Treating the underlying symptom often solves the problem (and can lead to testosterone boosts).
How many people are actually taking it?
TRT use is increasing. Substantially.
Between 2000 and 2011, TRT sales quadrupled while the diagnosis of testosterone deficiency stayed flat.
More recently, one study5 found that testosterone therapy grew significantly from 2018 to 2022. The biggest increase—120%—was among men under the age of 24 … people who, arguably, are already surging with testosterone.
Much of the rise can be attributed to tele-health clinics. Online purveyors run advertising around their product and deliver testosterone to your door. (Companies like Hone, Blokes, Hims, PeterMD, and—wait for this name—DudeMeds.)
These companies test your biomarkers and do a brief consultation. Then, in many cases, they prescribe TRT regardless of whether your levels are low or not.
The “secret shopper” study6, conducted by researchers at Northwestern University, found that 85 percent of online testosterone clinics gave a TRT prescription to a 34-year-old male with normal and healthy testosterone levels.
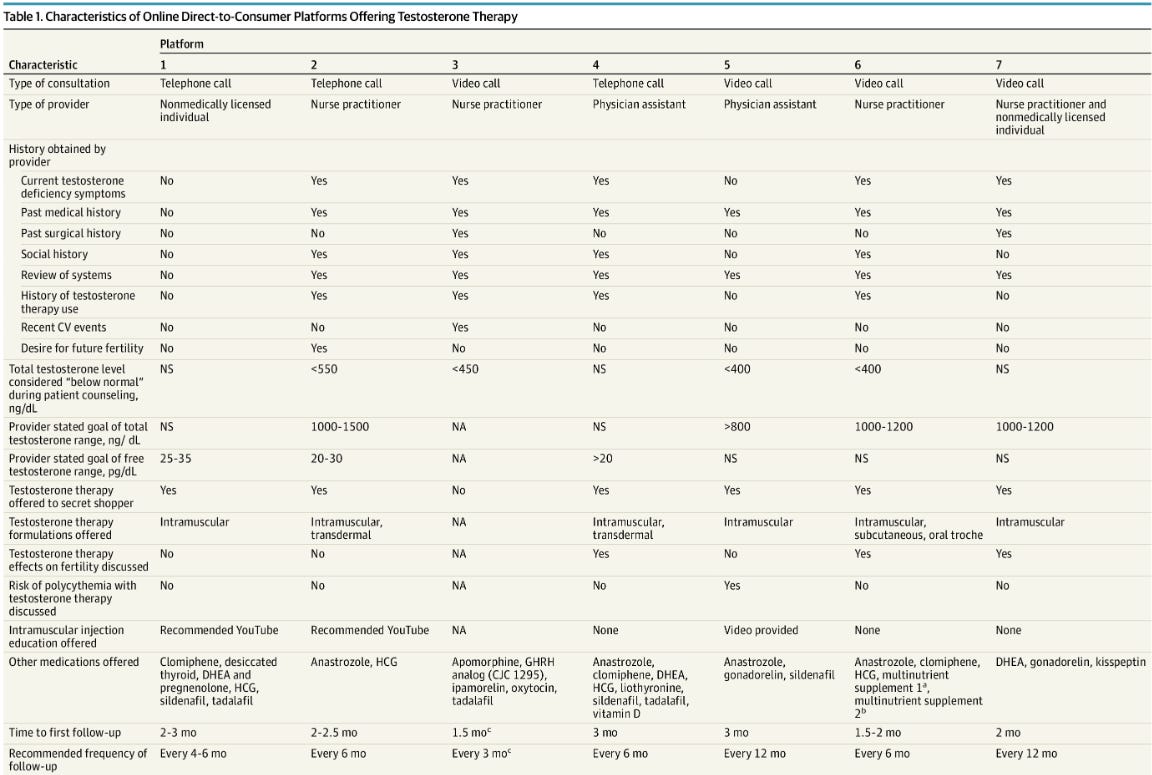
The Economist reported that just saying you’re tired, sad, or having trouble putting on muscle is enough to get the drug to your door.
Which sort of reminds me of how people get medical marijuana cards: Visit specific doctor. Say “I’m sad.” Weed doctor notes that weed often makes a person happy. Weed doctor then issues a medical marijuana card for a few hundred bucks.
It’s hard to know exactly how many men are using TRT. Some data from 2013 suggests 3.2% of men over 30 had a prescription. Given the rise in online clinics, I feel safe saying it’s between 4 and 5 percent of men.
Who does TRT help?
For its original targets, men with clinically low T and symptoms, it works fairly well.
For performance and vanity uses it also works—in the short term.
As we learned from Foster’s conversation, men will often feel great for a while—until they experience some downsides.
What are the downsides of TRT?
Downsides occur most often in men who start taking TRT while having relatively normal levels of testosterone.
As Foster’s anonymous friend noted:
Mood swings: anxiety, irritability, even depression (ironically).
Testicular shrinkage: because the body stops making its own testosterone.
Infertility: sperm production drops and often goes to zero.
Blood thickening: requires therapy to deal with.
Estrogen swings: this can mean bloating, nipple tenderness, or gynecomastia.
Worse sleep.
And once you take TRT, your body often stops producing testosterone naturally.
For men with a real deficiency, that’s fine—your body wasn’t producing much anyway. But for men who started with normal levels, coming off can be difficult, and in some cases, your body never fully rebounds.
This might be one reason why online clinics market so aggressively: Once you get a customer, you often have a customer for life.
When you take TRT without needing it, you often then need more drugs to manage side effects. I.e., you start with wanting more energy or muscle, but end up having a full-time job of managing your hormones.
There are also problems with a lot of the research that suggests TRT is safe. Some studies have concluded, for example, that TRT use is not associated with heart issues. But the studies are trash. Read Dr. Cifu’s analysis of one study here.
A key takeaway: We lack long-term data on how TRT use impacts younger and healthy men who take it for cosmetic, wellness, and performance reasons. We don’t know how it impacts their hearts, moods, thinking, fertility, and cancer risk in the long run.
Which brings us back to our anonymous source. He felt great on the drugs. And then he didn’t.
In this way, perhaps TRT is a bit like morphine.
If you have clinically low testosterone, you’re like a soldier who’s been wounded on a battlefield. Morphine is abundantly helpful!
But if you’re a normal person shooting morphine, you’ll have a good time for a while—but then you’ll probably start to rack up some problems.
Have fun, don’t die,
-Michael
Here’s a list of drugs the DEA considers steroids.
Rostom, M., Ramasamy, R., & Kohn, T. P. (2022). History of testosterone therapy through the ages. International Journal of Impotence Research, 34(7), 623-625.
Thirumalai A, Anawalt BD. Epidemiology of Male Hypogonadism. Endocrinol Metab Clin North Am. 2022 Mar;51(1):1-27. doi: 10.1016/j.ecl.2021.11.016. Epub 2022 Feb 8. PMID: 35216709; PMCID: PMC9136962.
Selinger S, Thallapureddy A. Cross-sectional analysis of national testosterone prescribing through prescription drug monitoring programs, 2018-2022. PLoS One. 2024 Aug 28;19(8):e0309160. doi: 10.1371/journal.pone.0309160. PMID: 39196907; PMCID: PMC11355536.
Dubin JM, Jesse E, Fantus RJ, et al. Guideline-Discordant Care Among Direct-to-Consumer Testosterone Therapy Platforms. JAMA Intern Med. 2022;182(12):1321–1323. doi:10.1001/jamainternmed.2022.4928
I’ve been on TRT since June. When I started I said something about it and found that there are like 5 other dads in my orbit also on it. Try your PCP first. I got a three month supply for 15 bucks. Don’t pay boutique rates unless you have to.
When I was in college, 1968 or 1969, if you went to the College clinic and told the Docs you were, whatever-tired, lack muscle, low libido (but nobody would admit to that!)-he would give you Dianobol! I never took the prescription and gave it away in the gym. I remember the guys that took it got bigger and stronger, but we're puffy and bloated looking. When they went off they lost all the gains. On the other hand, I had a friend go on the 30 day/30 pounds breathing squat regime (Ironman mag). He drank 1 gallon of milk a day, lots of peanut butter, eggs (at that time you could purchase 1 gal milk or 3 dozen eggs $1 each!). In about 6 months he probably gained 40 to 50#s, squat, bench went up 100s of #s. He became a beast! He worked very hard in the weight room to get those gains! So, the problems of steroids vs intelligent training is a recurring cycle through the years depending on "discovery" of solution by each generation. Basically, hard intelligent training vs quick, dubious gains that require a constant readjustment due to screwing with hormones. Hard intelligent work wins every time!